Conventional medicine
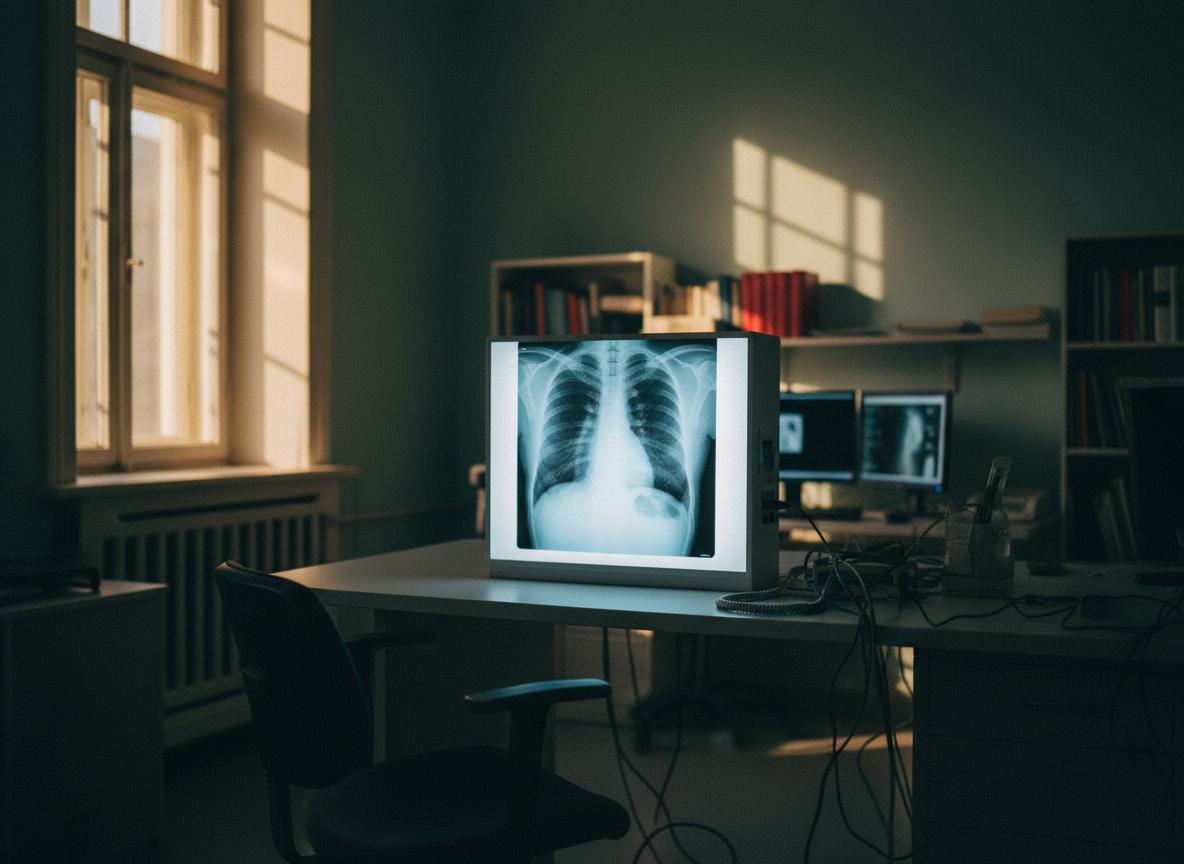
Classify the cough by duration (acute <3 wk, subacute 3-8, chronic >8). Image, run pulmonary function tests, and target the cause: post-infectious, asthma, GERD, post-nasal drip, COPD, or rarer (ILD, malignancy, heart failure).
Lung-health / breath-first
Once structural disease and asthma are excluded, much chronic breathlessness traces to dysfunctional breathing, mouth-breathing, low CO2 tolerance, poor air quality, and deconditioning. This track is mechanical, environmental, and behavioral.
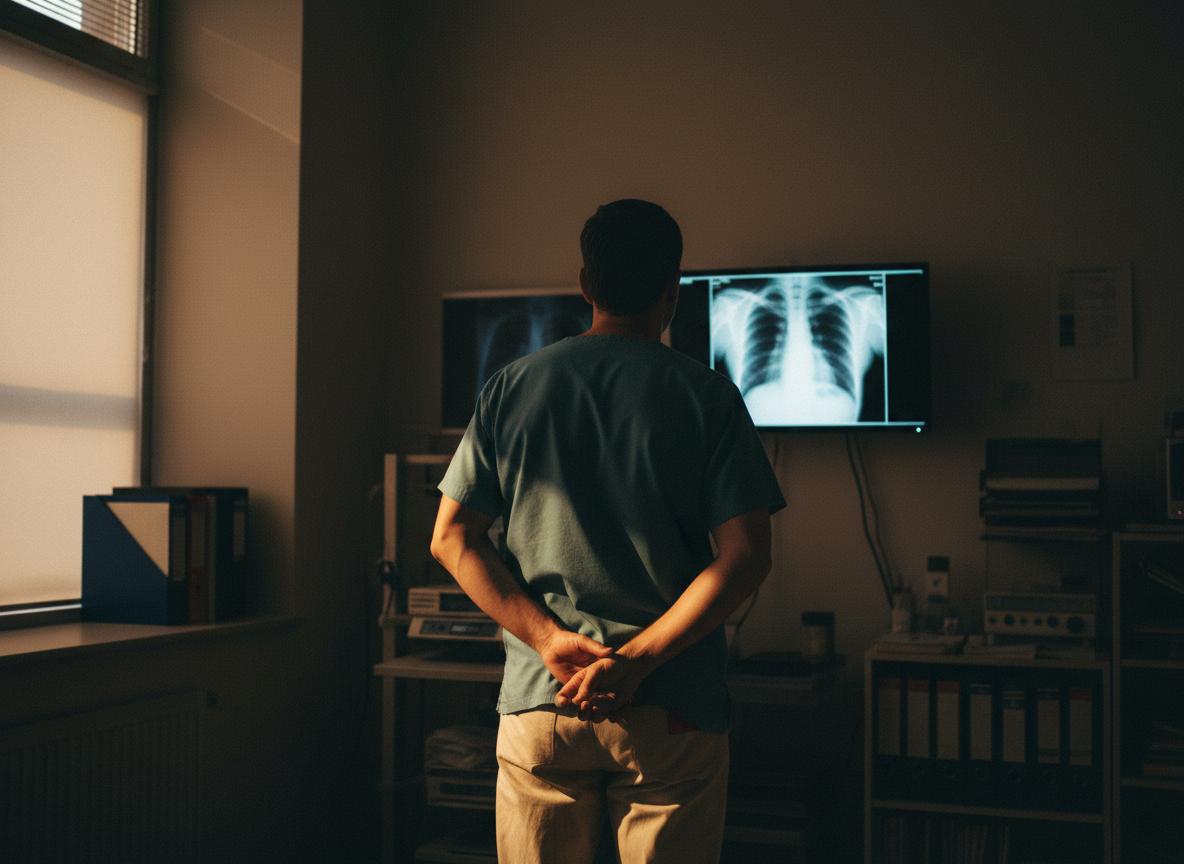
History, lung exam, vitals + SpO2. Red flags: hemoptysis, weight loss, fever, night sweats, leg swelling, dyspnea at rest → expedite. Otherwise outpatient workup.
Breath-first work starts AFTER imaging and PFTs are clean (or after asthma / COPD is medically managed). Any hemoptysis, weight loss, or acute dyspnea → medical care now.
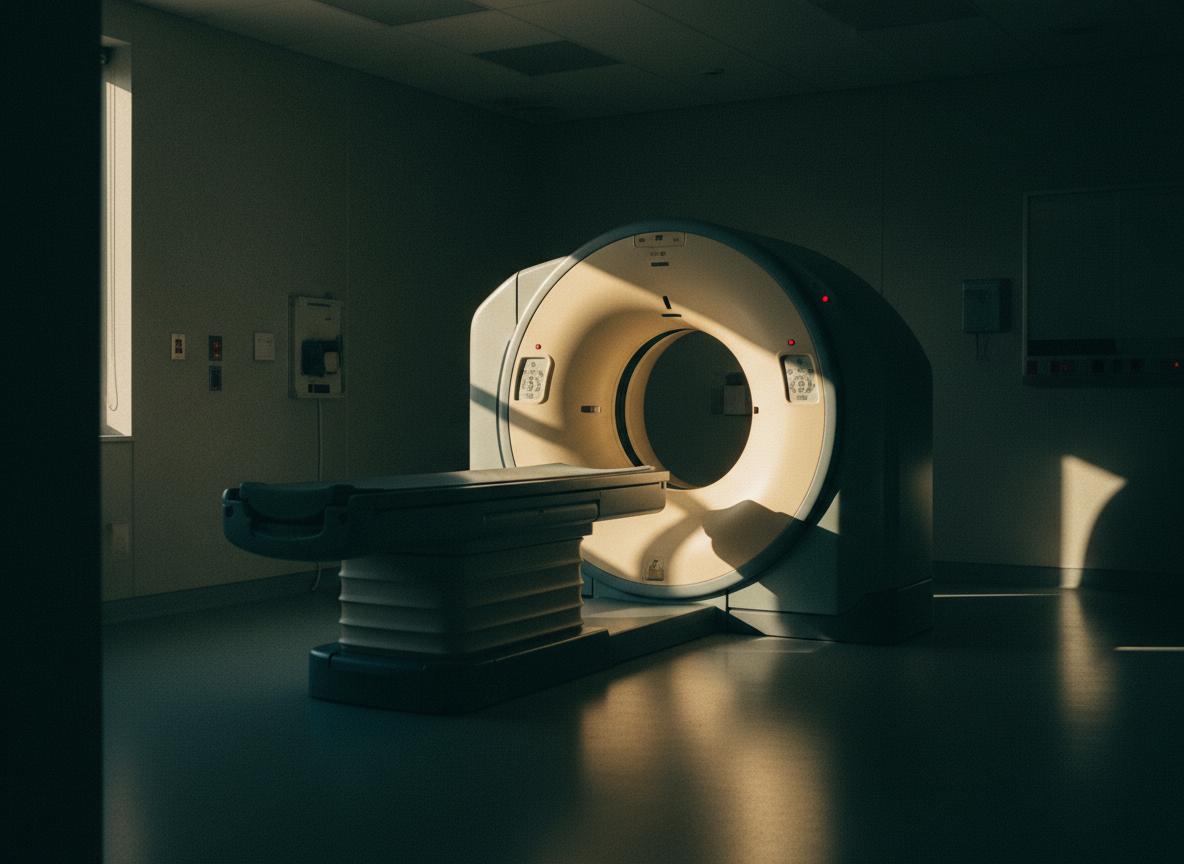
Chest X-ray first. Low-dose CT for high-risk smokers (LDCT screening), abnormal X-ray, or unexplained chronic cough.
BOLT score (control-pause). Switch to nasal-only breathing 24/7. Mouth tape at night. Long, light exhales, not bigger breaths. Identify chronic hyperventilation.
Spirometry pre/post bronchodilator (asthma vs COPD). Trial of inhaled corticosteroid / SABA, or PPI if reflux-cough suspected. Allergy / sinus workup if upper-airway.
Reduce indoor PM2.5: HEPA filter in bedroom, cooking vent on. Avoid scented candles, aerosols. Pet dander, mold (CIRS-style triggers), dust mite covers if positive on allergy testing.
Refractory or unexplained cough. Add: methacholine challenge, exhaled NO, induced sputum, bronchoscopy if indicated. Optimize asthma / COPD regimen.
Buteyko-style breath holds 2-4x / day. Nasal-only zone-2 cardio 3-5x / wk (45-60 min, can hold a conversation). Strength 2x / wk. Inspiratory muscle trainer optional.
Severe asthma biologics (omalizumab, mepolizumab, dupilumab). Pulmonary rehab for COPD/ILD. Oxygen if PaO2 ≤55 or SpO2 ≤88%.
Nasal breathing always. Weekly BOLT. Zone-2 3-5x / wk. HEPA + clean indoor air. Annual PFT if smoker history or family lung disease.
Every step has a price.
Here’s what we found.
We called clinics across Austin and pulled cash-pay quotes. Click any tile for the full provider list, phone numbers, and last-verified dates.



Who built
track B.
Breath researchers and exercise physiologists. Track B is for cleared, recurrent breathlessness or asthma already on medical management, not for unevaluated cough.

"Mouth-breathing is a slow-motion disease." Nose-only, slow exhales, mouth tape at night.
BOLT + CO2 tolerance training reduces breathlessness, exercise-induced wheeze, anxiety.

CO2 tolerance is trainable. Most chronic breathlessness is dysfunctional breathing, not lung disease.
Zone-2 cardio 3-5x / wk is the single most under-prescribed therapy in cardiorespiratory medicine.
- ACCP / ATS Cough GuidelinesSpecialty body
- GINA · Global Initiative for AsthmaGuidelines
- Cochrane · ICS for chronic coughSystematic review
- Patrick McKeown · Oxygen AdvantageButeyko practitioner
- James Nestor · "Breath"Author / journalist
- Brian Mackenzie · Shift AdaptBreath · performance
- Inigo San Millan · zone-2Exercise physiologist · UC